
The Deaths They Said Couldn’t Happen
From two teenage boys to 60 documented cases, the growing evidence of rare fatal vaccine reactions.

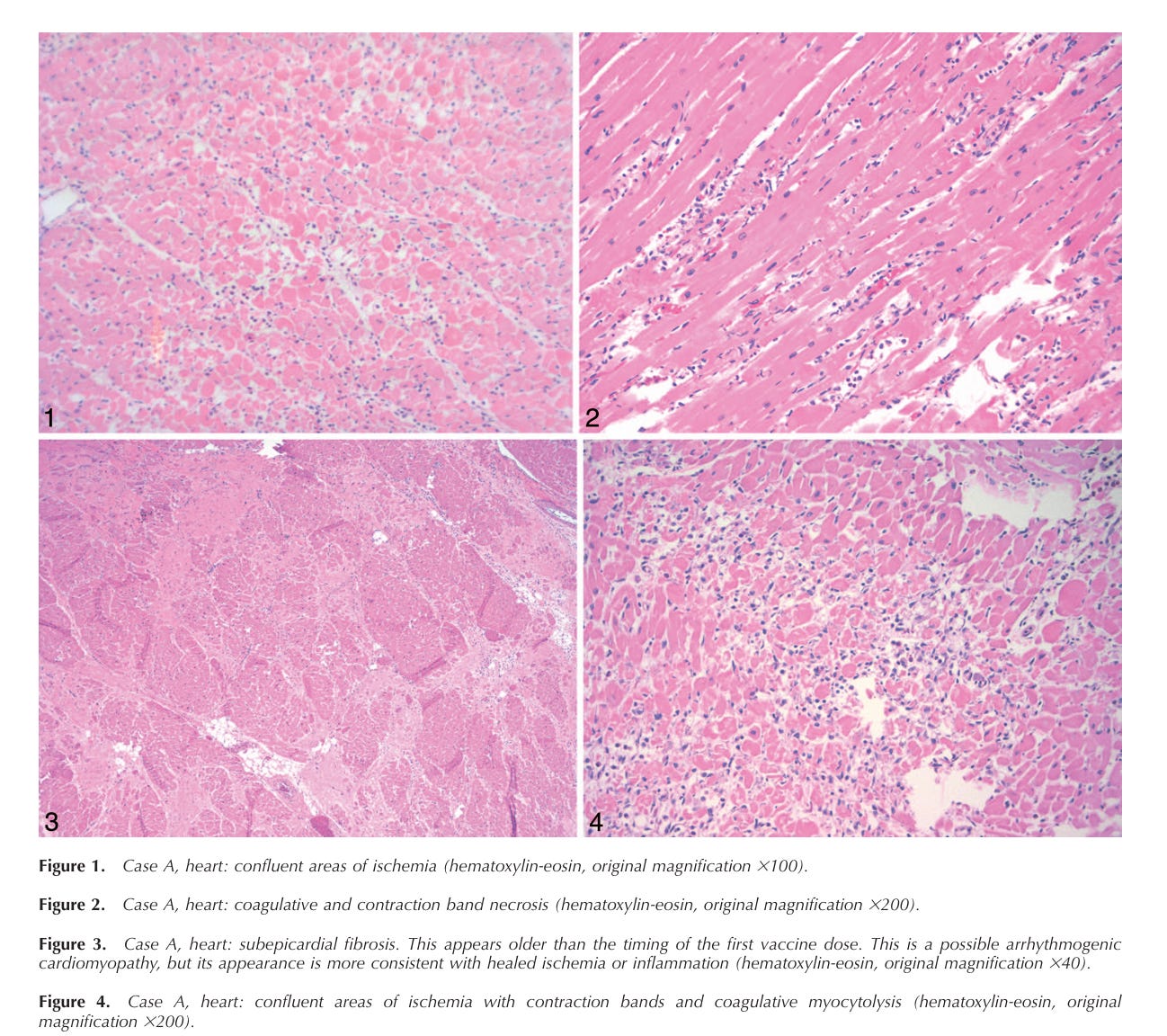
In the summer of 2021, two teenage boys went to bed and never woke up. Both had received their second Pfizer mRNA shots just days before—one three days earlier, the other four (link to case file). They were not frail or chronically ill; one was slightly overweight, the other was lean. There were no outward signs of heart disease. Yet on autopsy, their hearts showed a pattern of damage more akin to a stress-induced “broken‑heart syndrome” than classic viral myocarditis
Pathologists found contraction‑band necrosis and catecholamine‑type injury, not the lymphocytic infiltration that typifies traditional myocarditis. Both boys had died quietly in their sleep, their tragic fates uncovered only because the state’s chief medical examiner, Dr. James Gill, insisted on a detailed histopathological investigation.
The peer‑reviewed report on these two deaths made headlines among vaccine-safety researchers, but public‑health officials were quick to downplay its implications. The CDC countered with a letter suggesting alternative causes, even though those suggestions hinged on tenuous evidence. This tension—between the reality of documented, rare fatal outcomes and the reluctance of authorities to acknowledge them—runs through dozens of case reports from around the world. It underscores the need for honesty about the worst‑case scenarios so that doctors and parents can make truly informed decisions.
In what follows, you will find a catalogue of more than sixty published case reports detailing severe or fatal events temporally associated with COVID‑19 vaccination. These are not anecdotes from social media but peer‑reviewed investigations, autopsy findings, and transplant studies.

They show that vaccine‑induced immune thrombotic thrombocytopenia (VITT), fulminant myocarditis, catastrophic brain inflammation and other serious reactions do occur, albeit rarely. When even mainstream outlets like The Atlantic acknowledge that “some children may have died” from the shots, it is past time for a candid conversationtheatlantic.com. Transparency about these rare tragedies is not fuel for anti‑vaccine hysteria; it is a prerequisite for restoring trust in public health.
VITT / THROMBOSIS / CVST
Vaccine-Induced Immune Thrombotic Thrombocytopenia (VITT) is a rare but highly aggressive autoimmune reaction in which the immune system creates antibodies that attack platelet factor 4 (PF4), triggering catastrophic clotting and simultaneous bleeding. These cases nearly always occur 5–20 days after adenoviral-vector vaccines (AstraZeneca, J&J). Although officials repeatedly described these cases as “rare,” the published literature reveals a clear, deadly, and mechanistically consistent syndrome with dozens of autopsy-confirmed fatalities. Many patients were previously healthy and deteriorated suddenly.
Aladdin et al. — A previously healthy patient developed a full-blown VITT reaction progressing to disseminated intravascular coagulation, with clotting and bleeding occurring simultaneously; despite treatment, the syndrome proved rapidly fatal.
Ali M et al. — Following a J&J vaccination, a patient developed severe thrombocytopenia and cerebral venous sinus thrombosis, culminating in extensive hemorrhage and death.
Al-Mayhani et al. — The first symptom of VITT in this patient was a major ischemic stroke, highlighting that VITT can masquerade as a primary neurological emergency rather than classic clot symptoms.
Bérezné et al. — Patient with VITT worsened dramatically after receiving heparin and platelet transfusion—treatments later contraindicated when the mechanism of VITT became understood—ultimately dying from uncontrolled clotting.
Bjørnstad-Tuveng et al. — A young woman died from explosive intracranial bleeding just a week after AZ vaccination; autopsy confirmed hallmark PF4 antibodies.
Centonze et al. — Donor death from VITT caused simultaneous cerebral and hepatic vein thrombosis; case also explored whether such organs can be safely transplanted.
Choi et al. — Korea’s first death from VITT involved intracerebral hemorrhage secondary to massive venous thrombosis and thrombocytopenia.
De Michele et al. — VITT caused a malignant, swelling stroke that progressed relentlessly despite aggressive neurosurgical intervention.
Douxfils et al. — A patient initially stabilized on IVIG but suffered delayed immune recurrence and rapid fatal clotting due to falling IgG neutralizing levels.
Fanni et al. — Autopsy showed a body riddled with microthrombi—lungs, liver, kidneys—providing one of the clearest pathological demonstrations of how VITT kills.
Gómez-Roldós et al. — Fatal intracerebral hemorrhage tied to VITT, with imaging and labs matching the now well-described syndrome.
Greenhall et al. — Review of organ transplantation from VITT donors, documenting the risks of microthrombi transfer to recipients.
Greinacher et al. — The landmark paper identifying VITT as a novel PF4-antibody syndrome; six of eleven early cases were fatal.
Guditi et al. — Another VITT donor death with widespread organ thrombosis; case stresses importance of donor screening.
Huang ST et al. — A patient developed severe myositis and rhabdomyolysis alongside VITT-like clotting abnormalities after AstraZeneca; condition escalated to compartment syndrome and death.
Jamme et al. — Classic fatal VITT with PF4 antibodies and widespread venous thrombosis culminating in brain herniation.
Jamme et al. (2) — Documented the first French deceased donor with VITT, raising transplant-safety questions.
Kaimori et al. — Pfizer dose triggered TMA-like (thrombotic microangiopathy) microclotting in heart, kidneys, adrenal glands; patient died within 48 hours.
Kamura et al. — Moderna vaccine led to rhabdomyolysis with multi-organ small-artery thromboses driven by complement activation; fatal despite maximal care.
Medić et al. — Fatal intracranial bleed in a patient with vaccine-induced thrombocytopenia; an atypical VITT presentation.
Rodriguez et al. — First fatal VITT related to J&J vaccine documented outside the U.S.; confirmed PF4 positivity.
Satomi et al. — Autopsy revealed myocarditis and thrombosis post-vaccine in a highly inflammatory pattern.
Schultz et al. — Norway’s first cluster of VITT deaths; catalyzed international warnings.
Scully et al. — Laboratory confirmation that vaccine-induced PF4 antibodies behave similarly to autoimmune heparin-induced thrombocytopenia.
Shimoyama et al. — First reported autoimmune factor XIII deficiency post-vaccine, leading to catastrophic bleeding.
Takikawa et al. — Pregnant patient with underlying antithrombin deficiency suffered fatal cerebral venous thrombosis after Pfizer.
Uzun et al. — Fatal VITT in a donor with microthrombi documented in kidneys and liver; implications for transplant suitability.
Valsecchi et al. — Recipient of liver from VITT donor developed anti-PF4 antibodies, demonstrating transferability concern.
van Bruchem et al. — Multi-national transplant outcomes from VITT donors; microthrombi frequently detected.
Wiedmann et al. — Case series with extremely high fatality rates from VITT-induced CVST.
Wolthers et al. — Fatal intracerebral hemorrhage 12 days post-AZ; classical VITT time window.
MYOCARDITIS (FULMINANT & FATAL)
Myocarditis following mRNA vaccination is typically mild, but in rare cases, a hyperacute immune-driven cardiac inflammation leads to arrhythmia, heart failure, or sudden death. Autopsies in several reports reveal lymphocytic, eosinophilic, or mixed inflammatory infiltration, with patterns distinct from viral myocarditis. Some teenagers and young adults died in their sleep with no preceding symptoms—underscoring the silent, unpredictable nature of severe myocarditis.
Ameratunga et al. — A previously healthy adult died from fulminant necrotizing eosinophilic myocarditis one day after Pfizer dose #1; autopsy indicated a hypersensitivity-like storm.
Choi et al. — Korean military-aged male collapsed suddenly; autopsy revealed myocarditis without fibrosis, consistent with ultra-acute immune attack.
Gill et al. — Two teenage boys died in their sleep days after Pfizer; hearts showed contraction band necrosis and stress-type injury, not typical myocarditis.
Hoshino et al. — 27-year-old man died from fulminant myocarditis after Moderna; heavy T-cell and macrophage infiltration identified.
Kim SH et al. — AstraZeneca-induced myocarditis rapidly progressed to cardiogenic shock requiring emergency heart transplantation.
McMillan N et al. — Post-vaccine myocarditis led to cerebral hypoxia and death; myocarditis was the initiating pathology.
Nassar et al. — Autopsy-proven myocarditis following vaccination with no infectious trigger.
Satomi et al. — Fatal myocarditis with coexisting inflammatory vascular lesions.
Schwab C et al. — Autopsy series showing consistent myocarditis patterns temporally linked to mRNA vaccines.
Ujueta et al. — J&J-associated lymphohistiocytic myocarditis; abrupt clinical collapse.
NEURO-INFLAMMATORY CONDITIONS (ADEM, AHEM, ENCEPHALITIS, MYELITIS)
These cases involve immune attacks on the brain or spinal cord, sometimes resulting in hemorrhage, seizures, coma, or sudden death. Some mimic multiple sclerosis; others resemble necrotizing encephalitis or aggressive ADEM. In several reports, patients were initially misdiagnosed because early symptoms (headache, confusion, numbness) were nonspecific.
Ancau et al. — Three patients developed acute hemorrhagic encephalomyelitis shortly after AZ; one died despite steroid therapy.
Ballout et al. — Series documenting new-onset CNS inflammatory disorders within days to weeks of mRNA vaccination; one fatal ADEM case included.
Choi et al. — Fatal intracerebral hemorrhage from vaccine-associated thrombosis.
Jeon YH et al. — 19-year-old soldier with undiagnosed MS died in sleep; autopsy revealed active and chronic demyelinating lesions temporally preceded by vaccination.
Kits et al. — 53-year-old man developed AHEM with antiphospholipid antibodies after second Pfizer; rapid coma and death.
Mörz (preprint) & Mörz (peer-reviewed) — Autopsy revealed multifocal necrotizing encephalitis and myocarditis after mRNA vaccine; spike-protein immunostaining suggested immune trigger.
Nakano et al. — Fatal acute transverse myelitis developing shortly after Pfizer; extensive spinal cord inflammation.
Nimkar et al. — Autopsy-confirmed ADEM with widespread demyelination following vaccination.
Perez — Describes 26 rapidly progressive CJD-like neurodegenerative deaths occurring soon after vaccination; raises prion-like mechanistic questions.
Takahashi et al. — Rare case of aortic dissection with immune pericarditis/myocarditis following vaccination, showing multi-system inflammation.
When you have a trillion dollar empire to protect, the fact that people die from using your toxic products must be buried in a grave as deep as 1,000 miles. Endless profits is the goal, not longer lives. When they tell you to never question the safety and efficacy of vaccines, that is the signal that they are toxic and deadly garbage. If they were indeed safe and effective there would be mountains of trials and studies backing up that lie.
First, the CDC (or was it the FDA?) admitted recently that there were "6 provable Covid Jab related baby deaths", a day later, they admitted it was "10 Vax DEATHS". Now, a week later, we're reading that they now admit "60 documented VAX DEATHS". This is called 'drip feeding the truth' or a 'limited hang-out'!
I wish they'd get real and admit it's well into the thousands of Vax Related DEATHS from dangerous, unproven mRNA formulated Gene-Editing injections - they pretend are 'VACCINES'.
Hopefully, Kennedy will shut off Big Pharma's 'Get out of Jail FREE' card soon. The PREP Act was always designed to protect Big Pharma at the demise of the world's population. An insane 'law'!
Unjabbed Mick (UK Patriot!) We live longer!